
The Walsh Protocol: Undermethylation

The following content is extracted from a 650-page document that I personally authored in 2024–2025 and submitted to French researchers to present and analyze the Walsh protocol. The original manuscript was written in French, and I used automatic translation software to produce this English version. I solemnly swear on my honor that I am the sole author of this work, despite any appearance suggesting artificial intelligence involvement.
If you are here, it means that you want to learn about the Walsh Protocol, which I have mentioned in my live streams and other articles. I will once again explain what the Walsh Protocol is, based on the work of William Walsh, a well-known American biochemist.
This protocol is the culmination of more than 50 years of research and major discoveries on nutrients, genetics, behavior, and the role of nutrition in human health. It is based on the initial work of Carl Pfeiffer, a well-known American psychiatrist. The Walsh Protocol is the culmination of this work. It includes more than 30,000 patients, whose biochemical profiles have been analyzed in depth.
The protocol includes:
- 30,000 patients
- 110 markers tested for each patient
- 8,000 cases of ADHD and autism
- 8,000 cases of anxiety and depression
- Others.
In 1980, Carl Pfeiffer’s work was nominated for the Nobel Prize in Medicine on the same day that Walsh and Pfeiffer met. (He did not receive it). The protocol is a continuation of this work. Everything I will discuss in this article has been explained in the book “Nutrient Power,” published by William Walsh, which I invite you to read.
I hope you enjoy this article and that it helps you gain a clearer understanding of the mysteries of biochemistry and human behavior.
The biotype that I will study here is called “under-methylation”, a very distinctive and common biotype that can be the cause of anxiety and depression in people.
Undermethylation may be one of the most misunderstood biochemical patterns in modern psychiatry. On the surface, it can resemble classic depression, high-functioning anxiety, obsessive thinking, perfectionism, or chronic inner tension. Many individuals appear disciplined, driven, and mentally sharp — yet internally they struggle with persistent low mood, rumination, seasonal worsening, and a sense of emotional constriction.
What makes this pattern particularly complex is that it does not fit neatly into conventional diagnostic categories. It is not simply “low serotonin,” nor is it purely psychological. In the Walsh model, undermethylation reflects a reduced methylation capacity — a biochemical state that can influence gene expression, neurotransmitter balance, histamine regulation, and stress resilience. This may help explain why some individuals respond poorly to SSRIs, why certain forms of folate can aggravate symptoms, and why specific personality traits so often cluster together in these cases.
The most striking feature is the consistency of the profile. When properly identified, the pattern tends to follow predictable biochemical markers and predictable clinical responses. But it also requires precision. The wrong supplement can worsen symptoms. The right one, at the right dose, can produce steady and measurable improvement.
In the next section, we will examine the core biochemical markers of undermethylation, the characteristic symptom profile, and the structured nutrient protocol described in the Walsh model — including the common mistakes that can derail progress. In this episode of my Walsh Protocol series, you will learn more about histamine, gene involved in neurotransmitters activity, nutrients influencing methylation, personality traits that may be linked to biochemistry, as well as many other things.
I will also present a complete protocol to restore normal methylation status.
Starting today, I will be posting one episode of the Walsh Protocol every Monday. There are approximately 10 episodes left in this program.
Undermethylation: A Beginner-Friendly Introduction
If you are new to the concept of methylation, this may sound technical or intimidating at first. But the core idea is actually simple.
Every second, your body performs millions of tiny chemical reactions that regulate mood, focus, energy, and stress resilience. One of the most important of these processes is called methylation. I already did a small article about it here
In very simple terms, methylation is the transfer of a small chemical unit — called a methyl group (CH₃) — from one molecule to another. This small transfer has big consequences. It helps:
Produce neurotransmitters like serotonin and dopamine
Regulate gene expression (which genes are “turned on” or “off”)
Detoxify certain compounds
Support immune balance
Control histamine levels
When methylation functions properly, mood regulation tends to be more stable. When it is impaired or imbalanced, psychological and physiological symptoms may appear.
What Is Undermethylation?
Undermethylation refers to a state in which the body does not produce or utilize enough methyl groups efficiently. According to the clinical database developed by William J. Walsh and based on earlier work by Carl Pfeiffer, this is the most common biochemical subtype observed in their patients, representing roughly 40% of cases.
People in this category appear especially sensitive to the balance between methyl donors (like SAMe and methionine) and folates.
Interestingly:
They often improve with methyl donors.
They may worsen with high doses of folates.
They frequently show signs consistent with low serotonin activity.
This is not a psychiatric label. It is a biochemical pattern that may help explain why two people with similar depressive symptoms can respond very differently to the same supplement or medication.
Why This Matters for Beginners
If you have ever wondered:
Why do some people feel dramatically better on SAMe while others become anxious or overstimulated?
Why do SSRIs work very well for certain individuals but not others?
Why do some perfectionistic, high-achieving personalities struggle with inner tension and rumination?
The concept of undermethylation attempts to offer one possible biochemical explanation.
In the sections below, we will explore:
The biological markers of undermethylation
The typical personality traits associated with it
The response pattern to supplements and medications
And practical considerations for support
The goal is not to oversimplify complex psychiatry, but to provide a clear and accessible framework for understanding biochemical individuality.
Now that we have clarified the basics, let’s explore the profile of undermethylation in more detail.
Undermethylation: The Most Common Biotype
Understanding Undermethylation: Traits, Biochemical Markers, and Clinical Approach
In the Pfeiffer–Walsh database, undermethylation represents the largest patient group, accounting for roughly 40% of cases. According to the work of William J. Walsh and Carl Pfeiffer, this biotype is characterized by a strong sensitivity to the balance between methyl groups and folates in the brain.
People in this category tend to respond positively to methyl donors such as SAMe (S-adenosylmethionine) and methionine. However, paradoxically, they often react poorly to high doses of folates—even though folates are also involved in the methylation cycle. Walsh explains that the epigenetic effects of folates may override the simple presence of an attached methyl group (CH₃), leading to unexpected clinical reactions in susceptible individuals.
Most undermethylated patients display symptoms consistent with low serotonin activity. Many report having responded well to SSRIs (selective serotonin reuptake inhibitors) in the past, which further supports the serotonin connection.
How Is Undermethylation Identified?
Diagnosis in the Walsh model typically involves:
Whole blood histamine levels above 70 ng/mL
A SAMe-to-SAH ratio indicating low methylation capacity (often SAMe < SAH)
Clinically, these individuals are often recognizable based on behavioral patterns and personality traits.
They are frequently described as:
Perfectionistic
Highly self-disciplined
On the obsessive-compulsive spectrum
Prone to seasonal allergies (high histamine)
Major Symptoms and Personality Traits
Below is a simplified overview for readers new to this concept:
Typical Clinical Features
Good response to SSRIs
Good response to antihistamines
Positive response to methyl donors (SAMe, methionine)
Poor tolerance to folic acid or high-dose folates
Mental rigidity (OCD tendencies, strong need for control)
Strong academic performance; perfectionism
Suicidal ideation may be present in depressive states
Family history of high academic or professional achievement
Frequent rumination about past events
High inner tension despite appearing calm
Often described as quiet or very composed
High libido
Competitive in sports
Defiant toward parental authority in childhood
Frequent seasonal allergies
Low pain tolerance
This profile is remarkably consistent across many reported cases in the Walsh database.
Clinical Research and SAMe: A Striking Observation
Before discovering the Walsh protocol, I had already reviewed numerous studies on nutrition and supplementation for anxiety and depression. One study that stood out was conducted by George Papakostas, examining SAMe as an adjunct treatment for depression.
In his sample, approximately 36% of patients responded positively to SAMe, which is the body’s primary methyl donor.
This percentage is interesting. It suggests that only a subset of patients benefit significantly from this compound—consistent with Walsh’s idea that methylation status determines response.
A recurring theme in patient testimonials is that:
Some individuals experience clear antidepressant benefits.
Others become overstimulated, anxious, or even hypomanic.
There are reports of manic or hypomanic switches following SAMe supplementation. For example, one individual described being severely depressed and bedridden, then after taking 800 mg/day of SAMe, suddenly launching into ambitious travel plans abroad within days.
This illustrates an important point:
SAMe is powerful.
When given to the wrong person, it may cause adverse or even severe effects.
When given to the right person—carefully and progressively—it can be extremely helpful.
Practical Considerations About SAMe
There are also formulation challenges:
SAMe tablets are typically enteric-coated because the molecule must survive stomach acid to be absorbed in the intestine.
Some intramuscular (IM) formulations are available in certain countries, including Italy.
The compound can be expensive and sometimes poorly tolerated.
An Alternative Approach: Creatine and Methionine
In my personal view, creatine may be a more practical and better-tolerated option for many patients.
Here is the reasoning:
SAMe is synthesized in the body from methionine.
Creatine synthesis consumes large amounts of methyl groups.
By influencing this system strategically, we may enhance endogenous SAMe production.
I developed a theoretical approach that combines:
Methionine supplementation
Creatine supplementation
The goal is to significantly increase the body’s own production of SAMe. I refer to this concept as:
“The Methylation Pincer”
This idea makes sense primarily within the framework of the homocysteine hypothesis and methylation cycle dynamics. By combining methionine (a precursor) and creatine (which interacts with methyl demand), the body may upregulate methylation capacity more efficiently.
However, this approach must be used cautiously and progressively, with appropriate cofactors and clinical monitoring.
A Historical Note
As an example, Carl Pfeiffer used methylation-based strategies in certain cases of schizophrenia. The protocol varied depending on biochemical subtype, but methyl donors were part of his therapeutic toolbox in specific undermethylated patients.
This example is provided for illustration only. Methylation treatment must always be individualized.
Homocysteine and Undermethylation
Most undermethylated patients present with normal homocysteine (HCY) levels at baseline.
However, supplementation with:
SAMe
Methionine
tends to increase blood homocysteine.
For this reason, it is generally recommended to normalize homocysteine levels beforeinitiating aggressive methylation therapy.
In clinical practice, several weeks of:
Vitamin B6
Serine
are often sufficient to bring homocysteine back into an acceptable range.
According to clinical experience from the Walsh Research Institute, undermethylated individuals also tend to be intolerant to:
High-dose folates
Nutrients that increase SERT expression (e.g., choline)
Manganese
DMAE
Copper
These substances may worsen symptoms in this specific biochemical profile.
When Undermethylation and Pyroluria Overlap
A significant proportion of undermethylated patients also show elevated urinary kryptopyrroles, placing them in two biochemical categories simultaneously:
Undermethylation
Pyroluria
This combination is often associated with:
Severe anxiety
Very low stress tolerance
Heightened emotional instability
Since both conditions are associated with low serotonin activity, depressive and anxiety symptoms may be more intense.
These individuals are considered at higher risk for suicidal behaviors, particularly when anxiety is dominant. Severe anxiety can accelerate emotional decompensation.
In such cases, higher doses of vitamin B6 (typically 200–400 mg of P-5-P), combined with magnesium, are often required to restore serotonin synthesis.
Histamine and Undermethylation: A Two-Way Relationship
To understand undermethylation, we must understand histamine.
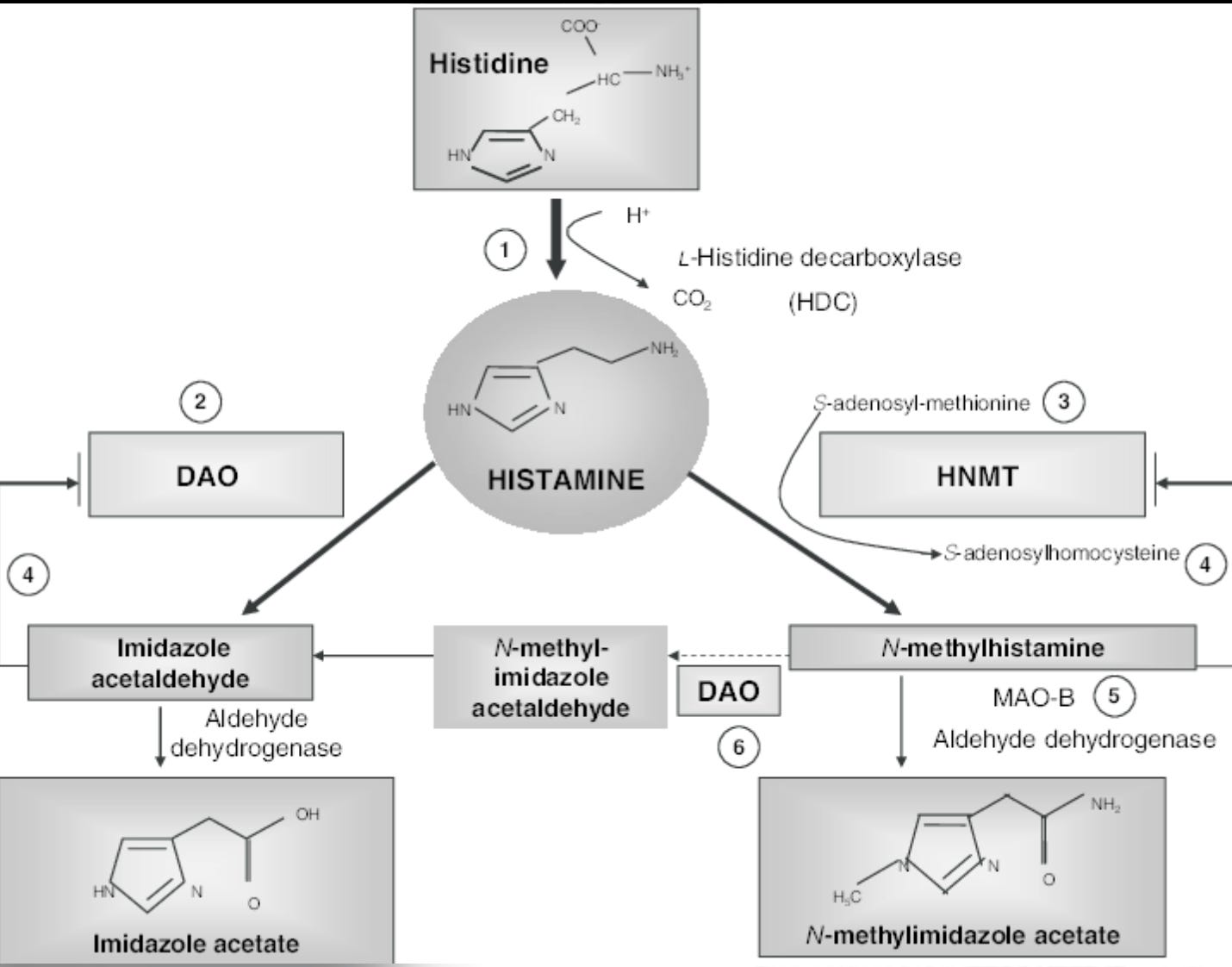
Histamine levels are highly sensitive to methylation status. The enzyme responsible for breaking down histamine in the brain is:
Histamine-N-Methyltransferase (HNMT)
This enzyme depends directly on SAMe, the body’s main methyl donor.
Basic Reaction
Methionine → (B9, B12, B6) → SAMe
↓
Histamine + SAMe → N-Methyl-Histamine (inactive)In simplified form:
If SAMe ↓ → HNMT activity ↓ → Histamine ↑When methylation is low:
The body cannot provide enough methyl groups.
HNMT activity drops.
Histamine accumulates in the blood and brain.
This may result from:
Vitamin B9 deficiency
Vitamin B12 deficiency
Methionine deficiency
Genetic variants (e.g., MTHFR, COMT)
Low SAMe therefore reduces histamine clearance and contributes to both physical and psychological symptoms.
The Double Feedback Problem
The relationship between histamine and methylation is bidirectional — and this is where things become complex.
Low methylation → Histamine accumulation
Histamine accumulation → Further methylation impairment
Why?
If histamine levels rise significantly, the HNMT enzyme begins working at maximum capacity (Vmax). When histamine exceeds a certain threshold, the enzyme becomes saturated.
This is not a direct chemical blockage. It is a metabolic congestion phenomenon.
When HNMT is saturated:
Histamine is no longer cleared efficiently.
SAMe is consumed rapidly.
SAH (S-adenosylhomocysteine) accumulates.
And here lies the critical point:
SAH inhibits methylation enzymes.
The Vicious Cycle
High Histamine →
HNMT Saturation →
SAMe Depletion →
SAH Accumulation →
HNMT Inhibition →
Even More HistamineChronic elevated histamine can therefore lead to:
HNMT saturation
SAMe depletion
SAH accumulation
Progressive methylation impairment
As SAMe drops, the synthesis of monoamines (serotonin, dopamine, norepinephrine) declines.
This contributes to:
Anxiety
Depression
Chronic stress sensitivity
And stress itself triggers mast cells to release more histamine.
Which closes the loop.
This biochemical feedback system helps explain why some patients feel trapped in cycles of anxiety, histamine intolerance, and depressive symptoms.
Methionine (SAMe): The Body’s “Natural SSRI”?
According to the epigenetic framework proposed by William J. Walsh, methionine plays a regulatory role in serotonin transporter expression (SERT).
In simple terms:
Higher methylation capacity may reduce SERT expression.
Reduced SERT activity means less serotonin reuptake.
Less reuptake means more serotonin remains in the synapse.
This mechanism resembles, in effect, how SSRIs function — but through a biochemical modulation pathway rather than direct receptor blockade.
Simplified Model
Methionine / SAMe ↑
↓
SERT expression ↓
↓
Serotonin reuptake ↓
↓
Synaptic serotonin ↑In the Walsh protocol, individuals transitioning off SSRIs were sometimes placed on:
Moderate-dose vitamin B6 (~300 mg/day)
Antioxidant support
Higher-dose methionine
Over several weeks (often 1–2 months), hypo-serotonergic symptoms reportedly improved gradually.
Importantly:
Methionine and SAMe are not only linked to serotonin.
They also influence dopamine pathways.
Unlike classical SSRIs, which mainly affect serotonin, adequate SAMe supports the synthesis of all monoamines, including:
Serotonin
Dopamine
Norepinephrine
This broader impact may explain why some patients experience improvements in motivation and drive — while others, if improperly matched, may become overstimulated.
A Final Word of Caution
These mechanisms are powerful.
SAMe and methionine are not benign “mood boosters.” They directly influence:
Epigenetic regulation
Neurotransmitter synthesis
Histamine metabolism
When correctly matched to an undermethylated individual, they may be highly beneficial.
When misapplied, they may destabilize mood.
Understanding the biochemical terrain is therefore essential before intervening.
Methylation is not just a pathway — it is a regulatory hub at the intersection of mood, immunity, stress, and gene expression.
Undermethylation, Histamine, and the “Natural SSRI” Concept
A clearer and more natural explanation for beginners
One detail that strongly caught my attention concerns the response rate to SAMe.
In a clinical study conducted by George Papakostas, about 36% of depressed patients responded positively to SAMe. In the Walsh–Pfeiffer clinical database, roughly 40% of patients are classified as undermethylated.
Two completely different investigative approaches — one psychiatric and pharmacological, the other biochemical and orthomolecular — arrive at nearly the same proportion of responders. The methods were different, but the percentage is strikingly similar. This convergence is not proof, but it suggests that methylation status may explain why only a subset of patients improve with SAMe.
That observation alone deserves attention.
Homocysteine: An Important Safety Consideration
Most undermethylated patients have normal homocysteine (HCY) levels at baseline. However, when we introduce SAMe or methionine, homocysteine can increase.
Why?
Because methionine is upstream in the methylation cycle. When you push methylation with methionine or SAMe, you can temporarily increase homocysteine production. For that reason, it is generally wise to stabilize homocysteine before beginning methylation therapy.
In practice, several weeks of vitamin B6 (often combined with serine) are usually sufficient to normalize homocysteine levels. Once HCY is in a safe range, methyl donors can be introduced more cautiously.
Clinical experience from the Walsh Research Institute has repeatedly shown that undermethylated individuals tend to be intolerant to:
High-dose folates
Nutrients that increase SERT expression (such as choline)
Manganese
DMAE
Copper
These compounds may worsen symptoms in this specific biochemical subtype.
When Undermethylation and Pyroluria Overlap
A significant portion of undermethylated patients also present with elevated urinary pyrroles (pyroluria). When these two patterns coexist, symptoms tend to be more intense.
Both conditions are associated with low serotonin activity. When combined, they often produce:
Severe anxiety
Very low stress tolerance
Heightened emotional reactivity
These individuals are often among the most vulnerable in clinical settings. When anxiety dominates, the risk of suicidal behavior increases — not necessarily because of deeper depression, but because severe anxiety can accelerate emotional breakdown.
In such cases, restoring serotonin function may require relatively high doses of vitamin B6 (often 200–400 mg of P-5-P) along with magnesium. The nervous system in these individuals is typically under significant biochemical strain.
Histamine and Methylation: A Two-Way Trap
To understand undermethylation fully, we must understand histamine.
Histamine is not only involved in allergies — it is also a neuromodulator in the brain. Its degradation depends heavily on methylation.
The key enzyme responsible for breaking down histamine in the brain is Histamine-N-Methyltransferase (HNMT). This enzyme requires SAMe — the body’s main methyl donor — to function properly.
In simple terms:
Methionine → (with B6, B9, B12) → SAMe
SAMe + Histamine → N-methyl-histamine (inactive form)
If SAMe levels drop, HNMT activity declines. When that happens, histamine accumulates.
This can occur due to:
Folate or B12 deficiency
Methionine deficiency
Genetic variants (such as MTHFR or COMT)
Chronic stress
But here is where the situation becomes more complex.
The relationship between histamine and methylation is bidirectional.
Low methylation increases histamine.
High histamine can further impair methylation.
When histamine rises significantly, HNMT begins working at maximum capacity (Vmax). If histamine continues to increase beyond what the enzyme can handle, the system becomes saturated. This is not a chemical “block” in the strict sense — it is metabolic congestion.
As histamine accumulates:
SAMe is consumed rapidly
SAH (S-adenosylhomocysteine) accumulates
SAH inhibits methylation enzymes
This leads to further reductions in SAMe availability.
The result is a vicious cycle:
High histamine → SAMe depletion → SAH accumulation → impaired methylation → even higher histamine
Over time, this can reduce the synthesis of monoamines such as serotonin and dopamine. And when serotonin drops, anxiety and rumination increase. Chronic stress then stimulates mast cells to release more histamine.
The loop reinforces itself.
This mechanism may explain why some individuals experience persistent anxiety combined with histamine intolerance and poor stress resilience.
Methionine and SAMe: The Body’s “Endogenous SSRI”?
Within the epigenetic framework described by William J. Walsh, methionine plays a regulatory role in serotonin transporter expression (SERT).
In simplified terms:
Increased methylation may reduce SERT expression.
Lower SERT expression means less serotonin reuptake.
Less reuptake means more serotonin remains available at the synapse.
Functionally, this resembles the mechanism of an SSRI — but achieved through modulation of gene expression rather than direct receptor blockade.
SAMe and methionine do more than influence serotonin. They also support dopamine synthesis. Unlike classical SSRIs, which primarily target serotonin, adequate methylation supports the production of all monoamines.
This broader mechanism may explain why some patients report improvements not only in mood, but also in motivation, drive, and cognitive clarity.
However, the same mechanism explains why others may become overstimulated or hypomanic if methyl donors are given inappropriately.
A Necessary Warning
SAMe and methionine are powerful metabolic regulators. They influence:
Gene expression
Neurotransmitter synthesis
Histamine degradation
Epigenetic signaling
When properly matched to an undermethylated individual, they may produce remarkable improvements.
When misapplied, they may destabilize mood.
Methylation is not a minor pathway. It sits at the crossroads of immunity, stress regulation, neurotransmission, and epigenetics.
Understanding this terrain is essential before attempting to modify it
Final Thoughts
Undermethylation, as described in the Walsh model, offers a compelling biochemical lens through which to view certain forms of depression, anxiety, OCD traits, and personality patterns.
However:
Methylation is complex.
Supplements like SAMe are powerful.
Biochemical individuality matters.
What works dramatically well for one person may destabilize another.
For newcomers, the key takeaway is simple:
Understanding methylation status may help explain why some people thrive on methyl donors—while others feel worse.
This model attempts to bring structure and predictability to those differences.
The content published on Feed Your Mind is provided strictly for educational and informational purposes. It does not constitute medical advice, diagnosis, or treatment under Articles L4161-1 et seq. of the French Public Health Code or under applicable U.S. law, and does not establish a doctor–patient relationship. In accordance with the U.S. Federal Food, Drug, and Cosmetic Act (21 U.S.C. § 301 et seq.), any discussion of nutrients or supplements is not intended to diagnose, treat, cure, or prevent any disease. The biochemical models and nutritional strategies discussed reflect research, clinical observations, and theoretical frameworks within nutritional psychiatry and remain subject to scientific debate. Readers are strongly encouraged to consult a licensed physician or qualified healthcare professional before initiating, modifying, or discontinuing any medication, supplement, or therapeutic intervention. The author and publisher assume no responsibility for decisions made based on the information presented.